Interoperability in Healthcare: From Concept to Capability
Interoperability has become one of the most frequently used — and least precisely understood — terms in digital health policy. With the European Health Data Space (EHDS) entering into force, interoperability is no longer a technical aspiration. It is becoming a legal and operational requirement.
But what exactly do we mean by interoperability? And why does it matter so much now?
Interoperability Is Not Compatibility — Nor Homogeneity
Interoperability is often confused with two related but fundamentally different concepts: compatibility and homogeneity.
Compatibility means that two systems can connect or exchange something under specific conditions. It is often bilateral and limited in scope.
Homogeneity means everyone uses the same system, the same software, the same model. While this may simplify integration, it is unrealistic at scale. Especially in Europe, where healthcare systems are decentralized and diverse.
Interoperability, by contrast, allows different systems, built by different vendors, in different countries, to exchange and use information in a meaningful way, without requiring them to become identical.
It is the ability of heterogeneous systems to:
- Exchange data
- Understand the meaning of that data
- Integrate it into workflows
Interoperability embraces diversity. It does not eliminate it.

The Levels of Interoperability in Healthcare
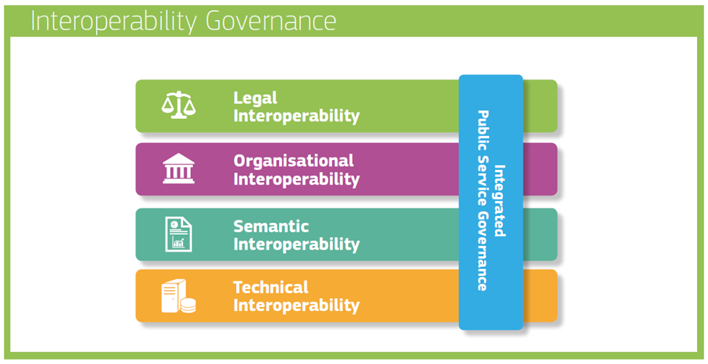
In healthcare, interoperability is not only about connecting systems. It operates simultaneously at four interdependent levels.
Technical interoperability allows systems to exchange data, through standards such as HL7, FHIR or DICOM. Without it, information simply cannot circulate.
Semantic interoperability ensures that the meaning of the data is preserved. Laboratory codes (LOINC), clinical concepts (SNOMED CT), diagnoses (ICD), or units (UCUM) must be interpreted consistently across systems. In healthcare, semantic ambiguity can lead to clinical risk.
Organisational interoperability aligns workflows, responsibilities, and governance. Exchanging a prescription or a discharge report implies agreed processes, validation rules, and accountability between institutions.
Legal interoperability provides the regulatory framework that authorises and structures data sharing. With the EHDS, interoperability becomes not only a technical objective but a legally framed obligation.
In healthcare, these four layers cannot function independently.
Data that moves but is misunderstood is dangerous.
Data that is well structured but cannot legally circulate remains unused.
Interoperability Exists in Many Domains
Healthcare is not the first sector to face this challenge.
Electricity
When you plug a device into a wall socket everywhere in Europe, you expect it to work. That reliability is not accidental. It is the result of shared voltage standards, plug formats, grid specifications, and safety norms. Countries may have different suppliers, but they follow common technical frameworks.
Telecommunications
Mobile phones work across borders because telecom operators adhere to common protocols (GSM, LTE, 5G standards). Without them, international roaming would collapse.
NATO
Military interoperability allows forces from different countries to coordinate operations. It requires agreed communication standards, procedures, command structures, and technical specifications. It does not require all armies to use identical equipment, but it requires structured coordination.
In each case, interoperability is built through:
- Agreed standards
- Governance structures
- Testing frameworks
- Training
Healthcare is now going through a similar transformation.

E-Health: A Fragmented Landscape
Healthcare digitalisation did not start with a common blueprint. Hospitals adopted information systems at different times, under different national policies, and often with local procurement logic. Vendors developed solutions tailored to specific markets. Clinical specialties built their own tools around their own needs.
The result is not a lack of digitalisation: it is a lack of coherence.
Across Europe, health information systems are:
- Built on heterogeneous architectures
- Using different data models
- Relying on partially overlapping terminologies
- Connected through custom interfaces or proprietary solutions
Two hospitals may both be “fully digital” and still be unable to exchange structured patient data in a usable way.
This fragmentation is not accidental. It reflects decades of decentralised investment, regulatory diversity, and rapid technological evolution. But it creates structural barriers to cross-border care, large-scale data reuse, and the effective implementation of the European Health Data Space.
Interoperability in healthcare is therefore not first about digitising more.
It is about aligning what already exists to enable the future.
The Standards Ecosystem: Many Use Cases, Many Frameworks
Healthcare interoperability is often discussed as if a single standard could solve the problem. In reality, the ecosystem is plural by necessity.
Different types of health data require different approaches. Exchanging a laboratory result is not the same as transmitting a medical image. Supporting clinical research does not follow the same logic as documenting bedside care. Each use case has generated its own frameworks, communities, and technical traditions.
Some standards focus on how data moves. For example HL7 (including FHIR) for structured exchange, or DICOM for imaging. Others focus on how data is structured and modelled, such as openEHR for detailed clinical content or OMOP for research harmonisation. Implementation frameworks like IHE do not create new standards but organise existing ones into coherent, testable workflows. Terminologies such as SNOMED CT, LOINC, ICD or UCUM ensure that data carries consistent meaning across systems and borders. In clinical research, CDISC structures data for regulatory-grade studies.
These frameworks are not competitors. They operate at different layers and for different purposes. The challenge is not choosing one over another: it is understanding how they complement each other within a coherent architecture.
The real complexity of healthcare interoperability does not lie in the absence of standards.
It lies in navigating an ecosystem where multiple standards coexist, overlap, and must be implemented together.
EHDS: A Regulatory Step Toward Legal Interoperability
The European Health Data Space (EHDS) introduces, for the first time, a common legal framework for health data exchange across Europe. Its objective is not to standardise all hospital data, but to define a harmonised baseline for specific priority use cases such as patient summaries, e-prescriptions, laboratory results or medical imaging reports. Through the European Electronic Health Record exchange Format (EEHRxF), EHDS structures how these data categories should be exchanged across Member States. Its ambition is to create a more homogeneous form of legal interoperability in Europe, ensuring that data sharing is not only technically possible, but legally aligned and enforceable across borders. However, the scope of EHDS remains narrower than the full complexity of hospital information systems. (See our detailed article on the EHDS framework here).
The Missing Piece: Skills
Europe does not lack interoperability standards. It lacks professionals trained to implement them coherently.
Applying FHIR is not just a development task. Using SNOMED CT is not just selecting a code. Implementing IHE profiles requires understanding workflows. Aligning with EHDS requires both technical and regulatory literacy.
Interoperability sits at the intersection of clinical practice, software engineering, data governance, and policy. Without structured education, even well-designed standards remain underused or inconsistently applied.
This is precisely where the XiA project intervenes. Rather than creating new standards, XiA develops educational content and structured learning pathways to build operational competence around existing frameworks, particularly those relevant to EHDS and the EEHRxF.
Because regulation can mandate interoperability.
But only skills can implement it.

Author : Luc Chatty